Is a Coccyx Injury Also a Concussion?
- paula8883
- Mar 27
- 5 min read
A Whole-Body Perspective on Impact, Dural Tension, Scarring, and the Brain
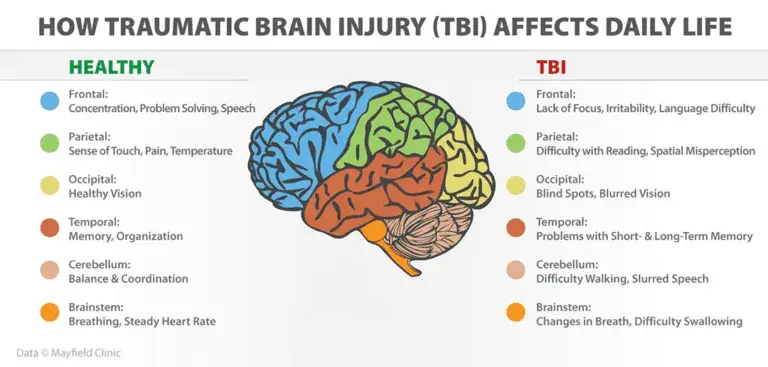
We usually reserve the word concussion for a direct or indirect force to the head that causes a mild or serious traumatic brain injury.
Modern concussion science shows that the injury mechanism is not simply “a bang to the skull,” but a complex biomechanical and neuro-metabolic event involving acceleration, deceleration, tissue strain, ionic disruption, energy crisis, autonomic change, inflammation, and altered network function in the brain. Rotational motion appears especially important in brain injury risk.
That matters when we think about falls onto the coccyx. It also matters when understanding our client and their experience.

A coccyx impact is usually treated as a local musculoskeletal injury. Yet anatomically, the coccyx is not isolated from the central nervous system.
. Anatomical studies describe this lower continuity as a real connective linkage between the distal spinal cord coverings, the dural sac, and the coccygeal region.
So when someone falls hard onto the tailbone, the question is not only “Did they bruise the coccyx?” but also “What happened to the tension, pressure, and signalling through the whole neuro-axis?”
That doesn't mean every coccyx injury should be diagnosed as concussion. The current evidence does not support that claim directly. What it does support is a more interesting and clinically useful proposition.
A coccyx injury may create a through mechanical force transmission, dural traction, altered spinal and cranial fluid dynamics, autonomic alarm responses, and compensatory guarding throughout the axial system.
There are some striking clues in the literature. Case reports describe cerebrospinal fluid leakage after sacral or coccygeal trauma, showing that lower-spinal impact can, in at least some cases, disturb the thecal or CSF system rather than remaining purely “local.” Those are unusual cases, but they make the broader point that distal trauma can have central consequences.
We also know from the upper cervical literature that the dura is mechanically linked to surrounding myofascial structures through the myo-dural bridge, and that these connections may help regulate dural tension and support cerebrospinal fluid dynamics.
That is highly relevant to concussion teaching, because it reminds us that the nervous system does not float in splendid isolation; it is mechanically embedded in connective tissue relationships from skull to sacrum.
Clinically, this gives us a much richer model. A fall onto the coccyx may trigger, headache, dizziness, visual strain, nausea, brain fog, emotional responses, poor balance, neck tension, altered breathing, pelvic floor overactivity, and a sense that the person “has never quite reset” since the fall.
If the impact occurred as a young person - later in life this can emerge as neck creptitis, vertigo, headaches, sinus issues, eyesight and hearing disturbance, temporo-mandibular presentations, balance, cognition and the two are not often connected when the client presents in clinic.
Some of those symptoms overlap with classic concussion presentations, while others reflect autonomic and mechanical adaptation. The overlap does not prove equivalence, but it does justify a broader assessment lens.
The image below is a schematic visual to demonstrate the global impact of a coccyx hit to the whole spine and skull -

From a clinical perspective, the role of the Bowen Technique in both concussion and coccyx-related presentations sits within its ability to influence the nervous system, fascia, and fluid dynamics simultaneously.
Rather than forcing structural change, Bowen uses gentle, precise inputs over key neuromuscular and fascial points to stimulate mechanoreceptors, which can down-regulate sympathetic overactivity and support parasympathetic recovery.
In concussion, where the neuro-metabolic cascade and autonomic disruption are central features, this creates an opportunity to reduce protective tone, improve coordination, and restore a sense of safety within the system in coccyx injury,
Bowen may help reduce sacral and pelvic floor tension, improve load distribution through the axial skeleton, and ease dural and fascial strain patterns that may be transmitting force cranially.
While high-level trials specific to Bowen in concussion are still emerging, its clinical value lies in its whole-system approach—supporting the body’s ability to reorganise after impact rather than treating the head or tailbone in isolation.
And this is where scar work becomes very important.
A coccyx injury rarely happens in a vacuum. Many people with persistent concussion-type symptoms also carry additional load in the system: sacral scars, pelvic scars, episiotomy scars, C-section scars, abdominal surgery scars, spinal surgery scars, or old impact scars elsewhere in the chain. MSTR describes scar tissue as capable of restricting fascial glide, biomechanics, circulation, and neural communication. That description is consistent with the broader idea that scars may act as chronic tension organisers within an already sensitised system, even though direct clinical trials of MSTR specifically for concussion recovery are still lacking.
A concussion is not only a brain event. It is often a brain–neck–dura–autonomic–fascial event. If the person has also had coccyx trauma, pelvic trauma, or significant scarring through the trunk, the clinician should consider whether those tissues are continuing to feed abnormal tension, protection, and sensory noise into the system. That is not an argument for replacing neurological assessment; it is an argument for completing it.
In other words: sometimes the head is where the symptoms shout, but the tailbone or the scar may be where the body is still whispering the story.

From a clinical perspective, the role of the Bowen Technique in both concussion and coccyx-related presentations sits within its ability to influence the nervous system, fascia, and fluid dynamics simultaneously.
Rather than forcing structural change, Bowen uses gentle, precise inputs over key neuromuscular and fascial points to stimulate mechanoreceptors, which can down-regulate sympathetic overactivity and support parasympathetic recovery. In concussion, where the neurometabolic cascade and autonomic disruption are central features, this creates an opportunity to reduce protective tone, improve coordination, and restore a sense of safety within the system.
For the client this is "joined up thinking" and can lead to unexpected positive health gains when the practitioner connects previous coccyx injuries with concussion type symptoms sometimes decades later.
If you are experiencing symptoms like these that are vague but bothersome in daily life and you know you have had a fall onto your tailbone in your lifetime - one that you remember as being siginificant . Follow the link below to find your local Bowen practitioner who can help you move past the experience into a more confortable life.
Reference list.
Giza CC, Hovda DA. The neurometabolic cascade of concussion. J Athl Train. 2001.
Giza CC, Hovda DA. The new neurometabolic cascade of concussion. Neurosurgery. 2014.
Tierney GJ, et al. Concussion biomechanics, head acceleration exposure and brain injury criteria in sport: a review. 2024.
Kleiven S. Why most traumatic brain injuries are not caused by linear acceleration but by angular head motion. 2013.
Ji S, et al. Head impact accelerations for brain strain-related responses in contact sports. 2014.
De Vloo P, et al. The filum terminale: a cadaver study of anatomy and histology. 2016.
Jiang Q, et al. Filum terminale: a comprehensive review. 2022.
Picart T, et al. Anatomical and histological analysis of a complex fascicular organization of the filum terminale. 2019.
Enix DE, Scali F, Pontell ME. The cervical myodural bridge: a review of literature and clinical implications. 2014.
Sun MY, et al. Utilization of MR imaging in myodural bridge complex investigation: a review. 2020.
Cawley DT, Power F, Murphy M. Cerebrospinal fluid leak after coccyx fracture. Spine J. 2016.
Foye PM, Singh R, Tangri V. Cerebrospinal fluid leak after fracture of the sacrum or coccyx. Spine J. 2019.
Cawley DT. Severe displaced fracture of the coccyx or sacrococcygeal junction causes trauma to the thecal sac. Spine J.2019.
McLoughlin Scar Tissue Release. What is MSTR? Official description of the technique.



Comments